The Question That Keeps Hospital Leaders Awake
Healthcare in India is in the middle of an aggressive expansion cycle. Hospital chains announce new facilities every quarter, private equity capital continues to flow into healthcare platforms, and tier-2 and tier-3 cities are positioned as the next growth frontiers.
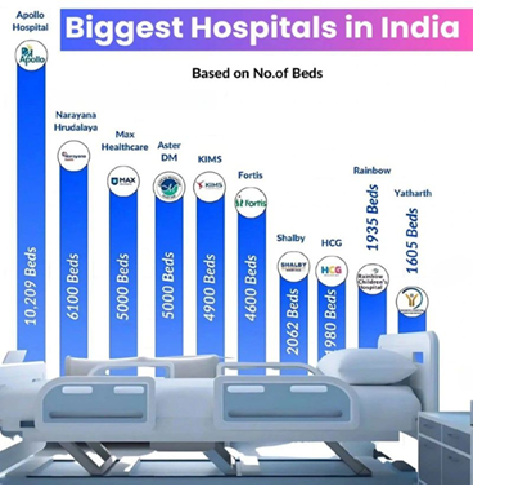
“ Private hospitals alone were expected to invest ~₹25,000 crore in capacity expansion and related capital expenditures during FY 25–26. ETHealthworld.com
Medium-term industry plans (FY 26–27) show ~₹30,000–₹32,000 crore capex being planned for adding ~14,500 beds across major hospital chains. The Economic Times+1”
Beds are added, specialties multiplied, footprints expanded, and topline revenues proudly reported. Growth, on the surface, appears inevitable—almost mandatory.
Yet the question that quietly keeps hospital promoters, CXOs, and investors awake at night is not how fast can we grow, but why does growth feel increasingly fragile?
This question emerges repeatedly across hospital diagnostics, board reviews, and expansion audits. Leaders chase visible symptoms—revenue growth, bed additions, new locations—while the root cause remains unaddressed: institutional fragility. Most hospitals do not fail because demand disappears. They fail because systems collapse under the weight of premature scale.
The contrarian truth is simple but uncomfortable:
Hospitals don’t fail because they grow slowly. They fail because they grow before they are ready.
This cornerstone article is written for hospital promoters, board members, CXOs, and healthcare investors who want to build institutions—not just add beds. It challenges popular growth narratives and explains why scale rewards some hospitals while breaking others. More importantly, it clarifies why hospital failure in India is rarely a clinical problem and almost always an institutional one.
Why Most Hospitals Fail: The Institutional Reality
Hospitals do not collapse because doctors lack competence or intent.
Clinical commitment is rarely the problem. Hospitals fail because healthcare is
one of the most complex institutional businesses to run—and complexity punishes
weak systems ruthlessly.
Five recurring institutional weaknesses appear long before visible
distress. These weaknesses are interconnected, reinforcing one another as scale
increases.
1. Growth Before Readiness
Early success creates confidence. A strong promoter reputation, a few rainmaker doctors, or a local brand advantage often drives rapid volume growth. Leadership assumes this momentum proves readiness for expansion.
But what works at 100 beds rarely works at 300. Informal coordination breaks. Decisions that once lived in the promoter’s head become bottlenecks. Processes multiply without discipline. Capacity expands faster than capability.
Scale does not correct immaturity—it amplifies it.
2. Weak Operating Discipline
Hospitals are operationally unforgiving. Patient flow, OT utilization, diagnostics, billing, discharge, pharmacy, manpower, and clinical coordination must function together every single day.
In many hospitals:
- i) Processes exist but are undocumented
- ii) Accountability is assumed, not defined
- iii) Performance depends on individuals, not systems
The result is operational unpredictability. Waiting times increase, length of stay drifts, staff burn out, and patient experience becomes inconsistent. Revenue may still grow, but control quietly disappears.
3. Capital Without Clarity
Access to capital is often mistaken for strategy. Debt or private equity becomes the justification for expansion instead of the outcome of readiness.
Hospitals invest heavily in infrastructure without clear ramp-up logic, cash-flow buffers, or working-capital discipline. EBITDA projections look attractive, but liquidity stress appears early. Many hospitals fail not because they are unprofitable, but because cash runs out before systems stabilize.
4. Fragile Trust and Brand
Hospital brands are built internally before they are experienced externally. Trust is created through consistency, not visibility.
When hospitals grow before trust is institutionalized:
- i) Patient confidence does not transfer
- ii) Doctor alignment weakens
- iii) Reputation becomes volatile
iv) Marketing spend increases, but credibility erodes.
5. Governance Gaps
Promoter-led decision-making works at inception. It fails at scale.
Without clear governance:
- i) Decision rights blur
- ii) Accountability weakens
- iii) Strategy becomes reactive
Operational issues are symptoms. Governance failure is the disease.
Hospitals rarely collapse suddenly. They bleed slowly—through margins, morale, leadership energy, and reputation—long before visible failure.
The Myth of Hospital Growth in India
In Indian healthcare, growth is often defined by visible metrics: number of beds, number of specialties, topline revenue, or geographic spread. These indicators are easy to communicate—to lenders, investors, peers, and sometimes to one’s own ego. Unfortunately, they are also deeply misleading.
True hospital growth is not about size. It is about predictability, repeatability, and institutional strength
Why Adding Beds Is Mistaken for Growth
Adding beds is capacity expansion, not capability building. A hospital can add 100 beds in a year, but it cannot build operating discipline, clinical governance, leadership depth, and financial predictability at the same speed.
Beds without systems don’t create value—they magnify inefficiency.
Without standardized processes, expansion increases variability in outcomes, cost leakages, patient dissatisfaction, and staff burnout. Many hospitals realize too late that more beds have only created more chaos.
Growth Pressure from Competition, Capital, and Ego
Hospital growth decisions are rarely neutral. They are driven by:
- Peer pressure: “Everyone else is growing—why aren’t we?”
- Capital pressure: Money becomes the reason to expand, not the enabler of strategy
- Emotional pressure: Legacy thinking, ambition, fear of missing out
Strategic growth demands restraint. It asks not can we grow, but are we ready to grow now?
When Expansion Works—and Why Big Players Get Away With It
A critical distinction must be made between large institutional hospital groups and regional or promoter-led hospitals.
India’s large hospital chains expand aggressively—and for them, this often makes sense. Their growth is not accidental. It is the outcome of years of deliberate institution-building.
They have already built:
- i) Institutional muscle: governance, professional management, decision discipline
- ii) Financial muscle: patient capital, predictable cash flows, balance sheet resilience
- iii) Operational muscle: standardized pathways, mature middle management
- iv) Brand muscle: national recall, insurer confidence, doctor pull
For these players, expansion is replication. Scale strengthens what already exists.
For smaller and regional hospitals, expansion is fundamentally different—and far more dangerous.
Growth Without Readiness Is the Most Expensive Mistake
Hospitals don’t collapse immediately after premature growth. They bleed slowly—through margins, morale, reputation, and leadership energy.
What Growth Readiness Actually Means
At AkoMentis, hospital growth readiness consistently rests on four non-negotiables:
- i) Operating discipline: documented, followed, audited processes
- ii) Doctor alignment: clarity on roles, incentives, authority, accountability
- iii) Financial clarity: predictable cash flows, cost visibility, working-capital control
- iv) Leadership bandwidth: managers who can run systems, not just fight fires
Without these, growth is not progress, it is risk multiplication.
Why Expansion Is Harder for Regional and Mid-Sized Hospitals
Growth for regional hospitals is not replication. It is reinvention under pressure. Large hospital chains expand by copying what already works. Regional and mid-sized hospitals expand while still figuring out what works. This difference is structural, not managerial—and it explains why the same growth playbook produces radically different outcomes.
1. Doctor-Led Fragility
What creates early success becomes the first scaling constraint.
Most regional hospitals are built around a strong doctor-promoter or a small group of clinicians whose personal reputation anchors patient volumes. In the first hospital:
- i) Clinical authority is centralized
- ii) Decision-making is fast and informal
- iii) Patient trust is personal, not institutional
This model works at small scale because proximity substitutes for systems. The promoter is visible, accessible, and perceived as the guarantor of quality.
When the hospital expands to a second or third location:
- i) The promoter cannot be physically present everywhere
- ii) Patient trust does not automatically transfer to a new site
- iii) Doctors at new locations interpret clinical standards differently
The result is clinical and cultural fragmentation. What was once a strength—centralized authority—becomes a bottleneck. Growth exposes the absence of codified clinical governance and leadership layers beneath the promoter.
2. Institutional Weakness
Presence is mistaken for process.
In many regional hospitals, systems exist but are:
- i) Informal
- ii) Person-dependent
- iii) Poorly documented
Processes live in people’s heads rather than in SOPs, dashboards, or governance routines. This is manageable when the organization is small and relationships are stable.
As scale increases:
- i) Decision rights become unclear
- ii) Standards vary by department or location
- iii) Conflicts increase between clinical, operations, and finance teams
Without institutional memory or documented processes, every new location reinvents decisions already made elsewhere. Scale does not hide these gaps—it amplifies them, leading to inconsistency, internal friction, and loss of control.
3. Financial Stress
Capital arrives faster than cash discipline.
Regional hospital growth is frequently funded through:
- i) High-cost debt
- ii) Short-tenure loans
- iii) Aggressive volume and ramp-up assumptions
Unlike large chains, regional hospitals lack balance-sheet resilience and patient capital. New facilities take longer to stabilize, but debt servicing begins immediately.
Common consequences include:
- i) Working-capital stress within the first 12–18 months
- ii) Pressure to push volumes at the expense of case mix or pricing discipline
- iii) Clinical and operational decisions distorted by cash urgency
Growth shifts from being a strategic choice to a survival imperative. Even hospitals that appear profitable on paper face liquidity stress because systems mature slower than financial obligations.
4. Branding Asymmetry
Trust does not travel at the same speed as infrastructure.
Large hospital chains carry:
- 1) National or multi-city brand recall
- 2) Insurer confidence
- 3) Doctor pull across geographies
Regional hospitals rely heavily on:
- 1) Promoter visibility
- 2) Local word-of-mouth
- 3) Community reputation
When they expand:
- 1) Brand equity does not transfer immediately
- 2) Ramp-up periods extend beyond projections
- 3) Marketing spend rises without proportional credibility gain
Patients may recognize the hospital name, but trust remains tied to individuals. Until institutional consistency is experienced repeatedly, brand perception remains fragile. This lag between physical expansion and trust transfer creates financial and reputational stress.
5. Leadership Bandwidth Collapse
Growth multiplies responsibilities faster than leaders can absorb them.
In many regional hospitals, a small leadership group:
- 1) Runs daily operations
- 2) Manages doctor relationships
- 3) Oversees finances
- 4) Drives growth strategy
This works at limited scale through personal involvement and extended working hours. Expansion increases complexity exponentially, not linearly.
As new units open:
- 1) Decision-making slows
- 2) Firefighting replaces planning
- 3) Strategic issues are deferred
Without a second line of capable leaders and clear delegation, leadership bandwidth collapses. The organization becomes reactive, and growth consumes leadership energy instead of freeing it.
The Underlying Pattern
Across all five segments, the same truth emerges:
Regional hospitals attempt to scale personalities, while institutions scale systems.
Until a hospital transitions from person-dependent success to system-dependent credibility, expansion will always feel risky, exhausting, and fragile.
Why Scale Amplifies Weakness, Not Strength
This leads to a fundamental truth: Scale rewards institutions. It punishes personalities.
Unless a hospital consciously transitions from doctor-centric prominence to institution-led credibility, scale will always feel risky.
Revenue Growth Is a Poor Indicator of Scalability. Revenue growth is seductive—and deceptive.
Hospitals often grow revenue through discount-led volumes, longer ALOS, or dependence on rainmaker doctors. Topline rises while margin quality and control quietly erode.
The real gap lies between cash and EBITDA, control and chaos. If outcomes and cash flows are unpredictable, growth is accidental.
The AkoMentis Staged Growth Framework
AkoMentis evaluates hospital scalability using a three-stage institutional framework:
Stage 1: Stabilize
Focus on operating discipline, cost control, predictable patient flow, and baseline governance.
Stage 2: Institutionalize
Build systems, middle management, clinical governance, and financial controls that reduce person-dependence.
Stage 3: Scale
Replicate proven systems across locations with capital discipline and governance oversight.
10-Point Growth Readiness Checklist
- 1. Documented SOPs across care continuum
- 2. Stable doctor engagement beyond individuals
- 3. Predictable monthly cash flows
- 4. DSCR consistently above 1.4
- 5. EMR adoption beyond billing
- 6. Standardized clinical pathways
- 7. Defined decision rights
- 8. Middle management depth
- 9. Insurer mix stability
- 10.Board-level review cadence
- If more than two items are weak, growth should pause.
Scalability KPI Table (Illustrative)
Dimension | KPI | Scalable Benchmark |
Operations | ALOS variance | <10% deviation |
Finance | Cash conversion cycle | <45 days |
Governance | Decision TAT | <72 hours |
Doctors | Revenue concentration | <25% on top 3 Specialty |
Growth | Ramp-up period | <18 months |
External Risks and Growth Strategies
Growth decisions in hospitals are shaped as much by the external environment as by internal readiness.
Even well-run hospitals operate within regulatory, payer, and market constraints that materially influence scalability. Ignoring these forces leads to expansion plans that look viable on spreadsheets but fail in execution.
Key External Constraints That Shape Hospital Growth
1. NABH Compliance Maturity
Accreditation is often treated as a certification milestone. In reality, it is a proxy for institutional maturity.
Hospitals with superficial NABH compliance:
- 1) Pass audits but lack embedded process discipline
- 2) Rely on documentation for inspections, not daily operations
- 3) Experience compliance fatigue as scale increases
As hospitals expand, inconsistent accreditation maturity across units
creates:
- 1) Variable patient experience
- 2) Clinical risk exposure
- 3) Operational drag
Growth magnifies compliance gaps. Hospitals that institutionalize NABH standards into daily workflows scale with lower friction than those that treat accreditation as episodic preparation.
2. Insurance Pricing and Payer Pressure
Insurance penetration in India has expanded faster than pricing
rationality.
Hospitals face:
- 1) Standardized package rates disconnected from cost structures
- 2) Delayed settlements impacting working capital
- 3) Limited negotiating power for regional players
As insurance volumes rise:
- 1) Revenue grows but contribution margins compress
- 2) Cash cycles lengthen
- 3) Pricing discipline erodes
Hospitals expanding without payer-mix strategy often discover that higher occupancy does not translate into healthier cash flows. Growth under payer pressure requires tight cost visibility and case-mix governance.
3. Uneven Bed Density and Demand Illusions
India’s bed density is uneven, not uniformly low.
While national averages suggest under-capacity, local realities vary
widely:
- 1) Urban clusters face saturation and intense competition
- 2) Tier-2 markets show demand volatility
- 3) Tier-3 markets require ecosystem building, not just beds
Hospitals expanding based on aggregate bed-gap narratives often misjudge:
- 1) Catchment maturity
- 2) Referral behavior
- 3) Ability to attract clinicians
Demand does not materialize automatically with infrastructure. It must be developed deliberately.
Strategic Growth Responses That Reduce External Risk
1. Market Development Before Greenfield Expansion
Build demand before building beds.
Market development involves:
- 1) Strengthening referral networks
- 2) Building specialty credibility
- 3) Establishing insurer relationships
- 4) Creating clinician pipelines
Hospitals that enter markets through OPDs, diagnostics, or partnerships:
- 1) De-risk demand assumptions
- 2) Shorten ramp-up periods
- 3) Preserve capital
Greenfield expansion without market development converts macro-opportunity into execution risk.
2. Selective M&A with Integration Discipline
M&A is often pursued for speed. Without integration discipline, it transfers problems at scale.
Successful hospital M&A requires:
- 1) Cultural compatibility assessment
- 2) Clinical governance alignment
- 3) Systems and data integration
- 4) Leadership continuity planning
Without these, acquisitions result in:
- 1) Parallel cultures
- 2) Financial opacity
- 3) Doctor attrition
M&A should be treated as institutional integration, not asset acquisition.
3. Asset-Light Expansion Models
Asset-heavy growth ties up capital before demand stabilizes.
Asset-light models—management contracts, clinical service partnerships, or lease-based setups—allow hospitals to:
- Enter new markets with lower capital exposure
- Test leadership and systems scalability
- Exit or recalibrate with limited balance-sheet damage
These models shift the focus from infrastructure ownership to institutional capability replication.
The Strategic Insight
External constraints do not block growth—they punish unprepared growth.
Hospitals that align expansion strategy with:
- 1) Regulatory maturity
- 2)Payer economics
- 3) Market realities
Scale with fewer shocks and greater predictability.
Technology and People as Growth Enablers
Technology enables scale only when adoption is deep. EMRs that stop at billing add little value. True scalability comes from clinical data, outcomes tracking, and decision support.
Equally critical are aligned incentive structures. Misaligned doctor incentives destroy institutional trust faster than capital shortages.
Proof from the Field: Case Snapshots
Aravind Eye Care demonstrates institutional replication through standardized processes and governance.
Manipal Hospitals illustrate how capital, governance, and professional management enable controlled scale.
SWOT for Regional Hospitals

Governance: The Final Gate to Scale, Capital is rarely the constraint. Clarity is.
Boards must ask:
- 1) Are systems stronger than individuals?
- 2) Is governance clear and enforced?
- 3) Is cash predictable—not just revenue?
- 4) Are doctors aligned beyond incentives?
- 5) Can this hospital run without heroic leadership?
If even one answer is unclear, growth should wait.
Closing Perspective
Hospitals don’t fail because they grow slowly. They fail because they grow before they are ready.
Scale is not a strategy. Institutional strength is.
At AkoMentis, we believe sustainable hospital growth is not chased—it is earned.